This site is intended for US healthcare professionals
In the Phase 3 trials SKYLIGHT 1 and 2 (pooled data) and DAYLIGHT, fezolinetant demonstrated improvements over placebo in Menopause-Specific Quality of Life (MENQoL) Total and Domain scores, and Patient Global Impression of Change in vasomotor symptoms (PGI-C VMS)
Pooled SKYLIGHT 1 and 2 data1
The below analyses do not control the type I error rate, i.e. without multiplicity adjustment, so p-values do not confer statistical significance. Rather, the p-values were used for the purposes of hypothesis generation.
Figure 1: Change from Baseline to Weeks 4 and 12 in MENQoL Total Scorea1
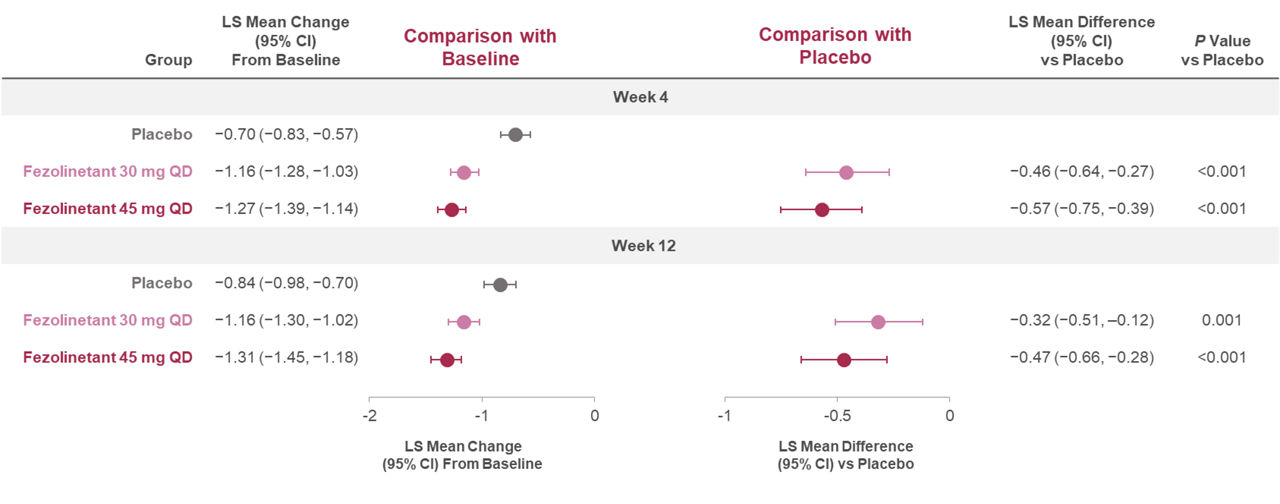
All randomized participants assessed according to the randomization at first dose (fezolinetant 30 mg n = 339; fezolinetant 45 mg n = 341; placebo n = 342). Negative change indicates an improvement from baseline. aComprises all four domains and 29 items. Adapted from: Cano A, BJOG 2024.
Figure 2. Change from Baseline to Week 12 in MENQoL Domain Scores1
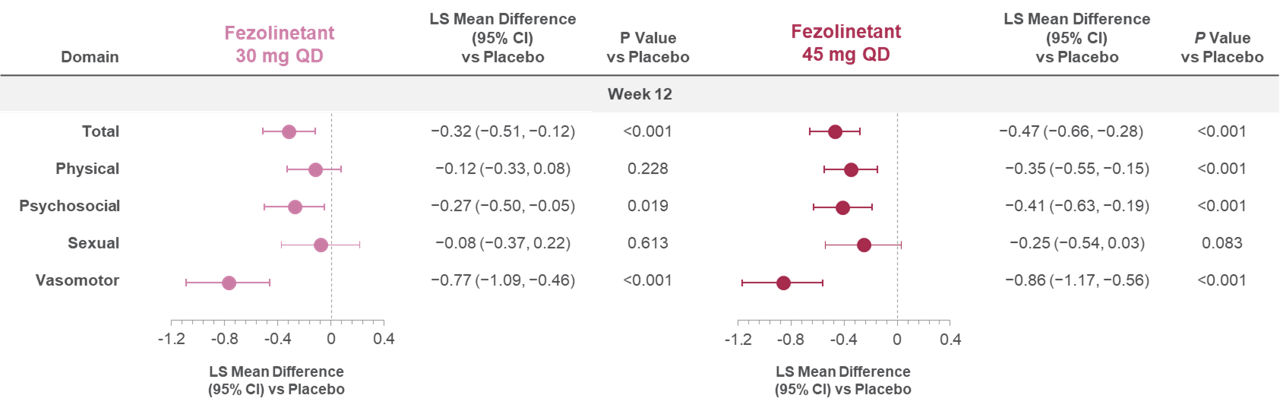
All randomized participants assessed according to the randomization at first dose (fezolinetant 30 mg n = 339; fezolinetant 45 mg n = 341; placebo n = 342). Negative change indicates an improvement from baseline. Adapted from: Cano A, BJOG 2024.
PGI-C VMS1
Figure 3: PGI-C VMS distribution at Week 4 and 121
Week 4:
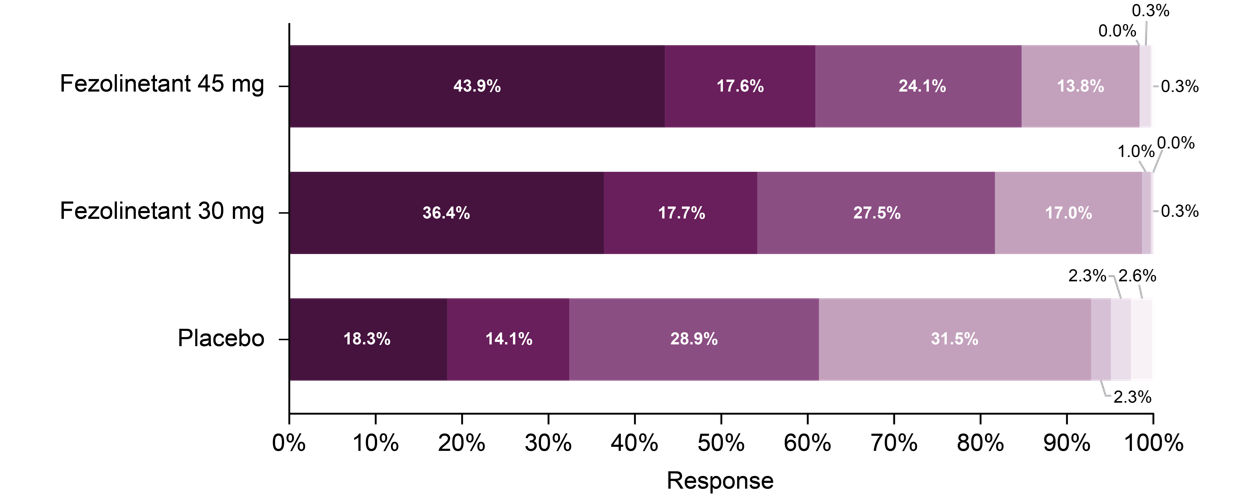
Week 12:
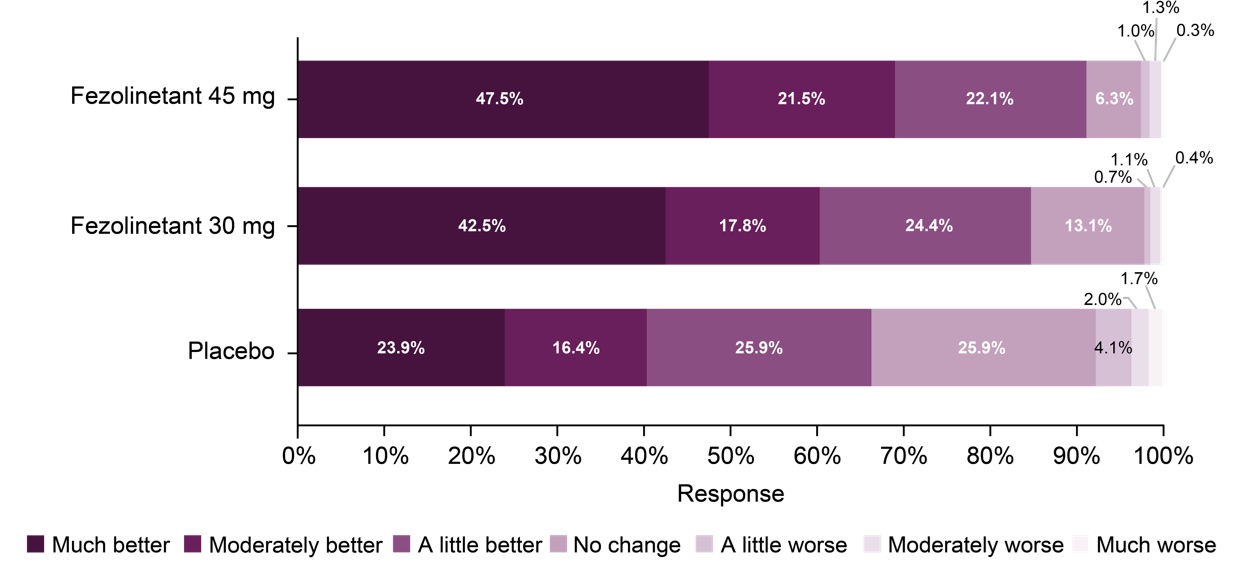
p < 0.001 for fezolinetant 30 mg versus placebo and for fezolinetant 45 mg versus placebo at Weeks 4 and 12. Pvalues were obtained using Cochran-Mantel-Haenszel test with modified ridit scores. Adapted from: Cano A, BJOG 2024
DAYLIGHT data2,6
The below analyses do not control the type I error rate, i.e. without multiplicity adjustment, so p-values do not confer statistical significance. Rather, the p-values were used for the purposes of hypothesis generation.
Figure 4. Change from baseline to Week 24 in MENQoL Total Scorea2
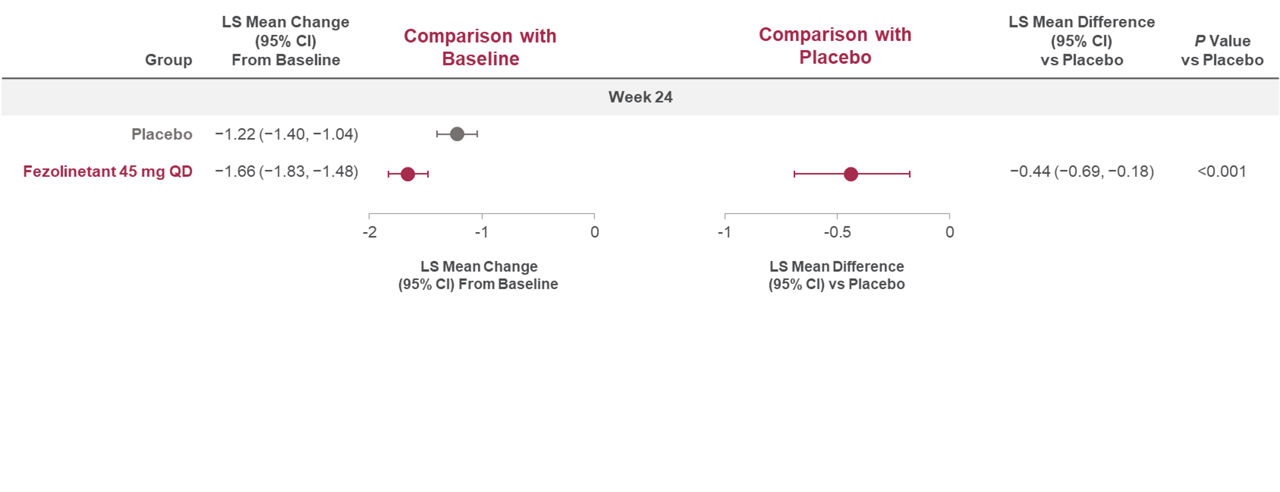
All randomized participants assessed according to the randomization at first dose (fezolinetant 45 mg n = 226; placebo n = 226). Negative change indicates an improvement from baseline. aComprises all four domains and 29 items. Adapted from: Shapiro M, Maturitas 2024.
Figure 5. Change from baseline to Week 24 in MENQoL Domain Scores2
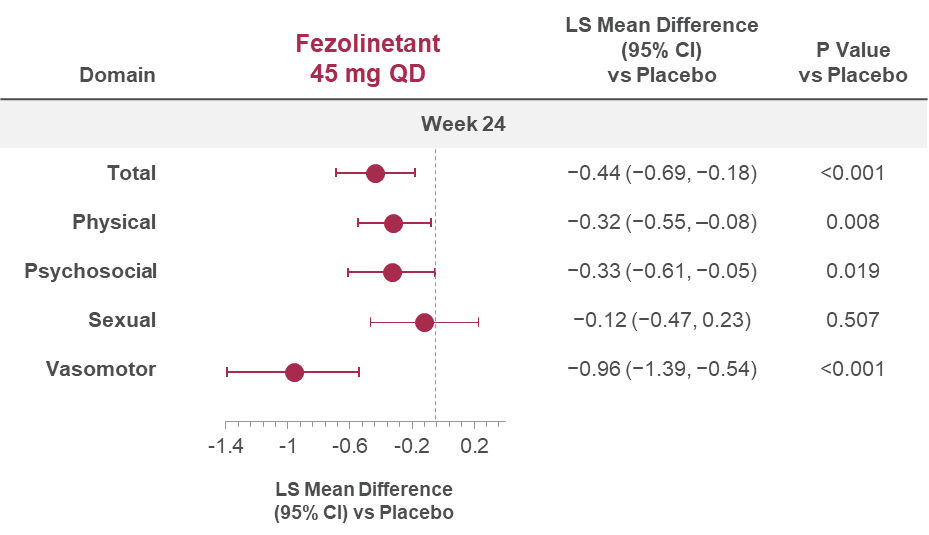
All randomized participants assessed according to the randomization at first dose (fezolinetant 45 mg n = 226; placebo n = 226). Negative change indicates an improvement from baseline. Adapted from: Shapiro M, Maturitas 2024.
Figure 6. PGI-C VMS distribution at Week 246
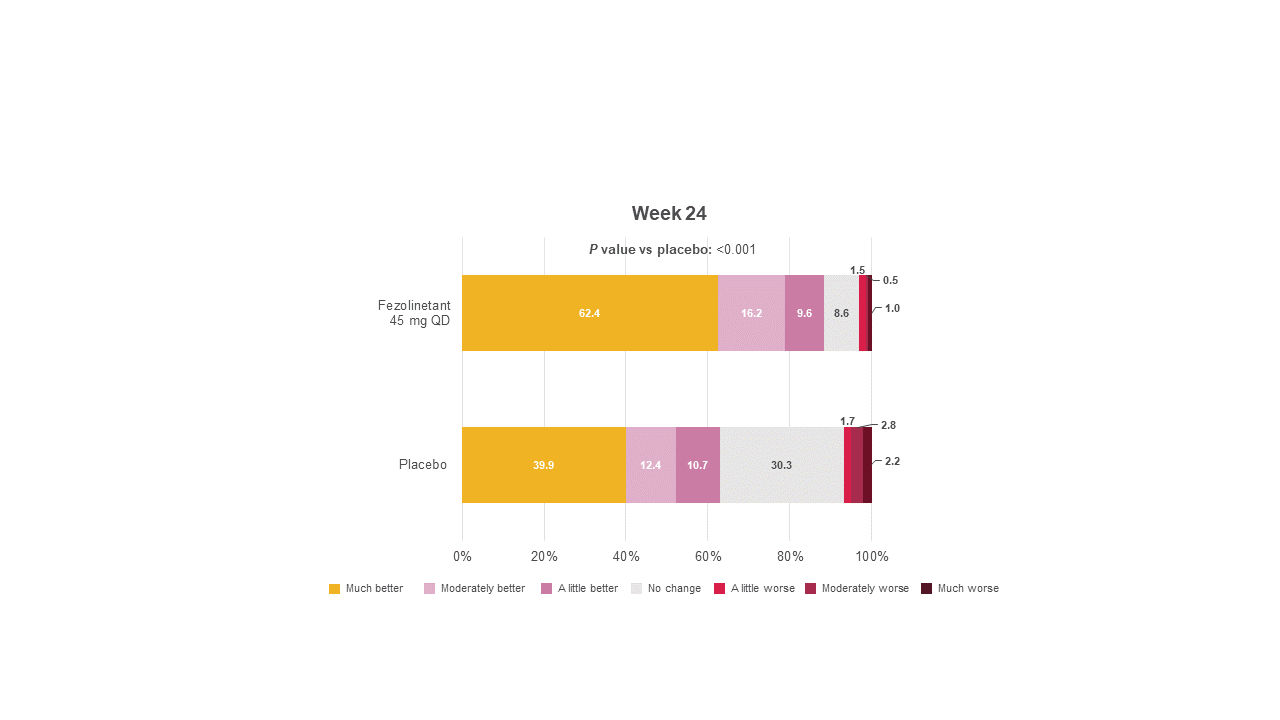
All randomized participants assessed according to the randomization at first dose (fezolinetant 45 mg n = 226; placebo n = 226). Adapted from: Schaudig K, BMJ 2024.
Phase 4 real-world study, OPTION-VMS, preliminary results3,4
Cano A, Nappi RE, Santoro N, et al. Fezolinetant impact on health‐related quality of life for vasomotor symptoms due to the menopause: Pooled data from SKYLIGHT 1 and SKYLIGHT 2 randomised controlled trials. BJOG: Int. J. Obstet. Gynaecol. 2024;131(9):1296-1305. Available at: https://doi.org/10.1111/1471-0528.17773.
C.M. MS, Wu X, Wang X, et al. Effect of fezolinetant on patient-reported quality-of-life outcomes: Data from a phase 3b study (DAYLIGHT) of the treatment of moderate to severe vasomotor symptoms associated with menopause in women considered unsuitable for hormone therapy. Maturitas. 2024;193108159. Available at: https://doi.org/10.1016/j.maturitas.2024.108159.
Neal-Perry G, Lederman S, Mancuso S, et al. OPTION-VMS: Preliminary Analysis of a Phase IV Observational, Real-World Study of Non-hormonal Pharmacotherapies for Bothersome Menopause-Associated Vasomotor Symptoms [poster]. The Menopause Society (TMS) 2025 Annual Meeting. Orlando, FL, USA. 2025.
Neal-Perry G, Mancuso S, Schild A, et al. Preliminary analysis of real-world effects of fezolinetant on menopause-specific quality-of-life vasomotor symptoms (MENQOL VMS) overall and by subgroups of interest: phase IV OPTION-VMS study [poster]. American College of Obstetricians & Gynecologists (ACOG) Annual Meeting. Washington, DC, USA. Poster #I23. 2026.
Thurston RC, Mancuso S, Helbing M, et al. OPTIONVMS: Preliminary analysis of a phase 4 observational, realworld study of nonhormonal pharmacotherapies for bothersome menopauseassociated vasomotor symptoms and depression and anxiety [poster]. Endocrine Society Annual Meeting (ENDO) 2026. Chicago, IL, USA. 2026.
Schaudig K, Wang X, Bouchard C, et al. Efficacy and safety of fezolinetant for moderate-severe vasomotor symptoms associated with menopause in individuals unsuitable for hormone therapy: phase 3b randomised controlled trial. BMJ. 2024;387(387):e079525. Available at: https://doi.org/10.1136/bmj-2024-079525.
Maki PM, Mancuso S, Helbing M, et al. Preliminary Analysis of Work Productivity Outcomes in OPTION-VMS: A Phase IV Observational, Real-World Study of Non-hormonal Treatment for Bothersome Menopause-Associated Vasomotor Symptoms [poster]. The Menopause Society (TMS) 2025 Annual Meeting. Orlando, FL, USA. 2025.
The medical information on this website is for educational purposes only and is intended to provide scientific information about Astellas products. This information is not intended as medical advice or clinical recommendations. This website is for use only by United States residents and licensed healthcare professionals (HCPs) practicing in the United States. Product labeling may vary between countries.
Please choose an option that best describes you:
For visitors outside the United States: click here


